Humans are not well adapted as beasts of burden. Heavy loads hung from the shoulders can really stress rib cage and spinal structures and cause thoracic outlet syndrome (Fig. 1).

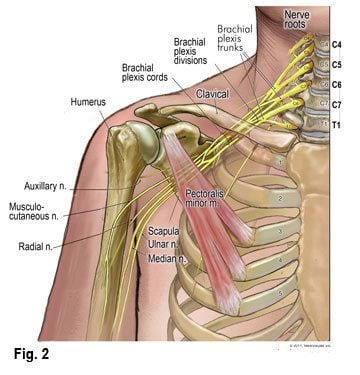
The generic term ‘thoracic outlet syndrome’ (TOS) is often used to describe a variety of symptoms associated with excessive frictioning of spinal nerves in the shoulder and brachial region. TOS involves compression, injury, or irritation to neurovascular structures at the root of the neck, upper thoracic region, or beneath the pectoralis minor muscle. Compression syndromes at these sites are primarily neurologic and involve the brachial plexus—most often the lower trunk or medial cord (Fig. 2).
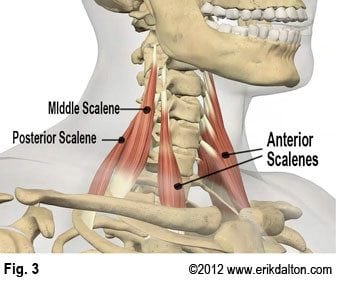
 Additionally, the subclavian artery and vein may also be compromised. Cervical nerves and vessels often become trapped between fibrotic anterior and middle scalene tendons as they enter the thoracic inlet (Fig. 3).
Additionally, the subclavian artery and vein may also be compromised. Cervical nerves and vessels often become trapped between fibrotic anterior and middle scalene tendons as they enter the thoracic inlet (Fig. 3).
 Prolonged scalene spasm from injury or overuse can also cause problems as they tug on the first rib pulling it up against a ‘drooping’ clavicle. When the brachial plexus gets squashed between the clavicle and rib, a condition known as costoclavicular syndrome arises. This disorder is thought to be one of the leading causes of TOS.
Prolonged scalene spasm from injury or overuse can also cause problems as they tug on the first rib pulling it up against a ‘drooping’ clavicle. When the brachial plexus gets squashed between the clavicle and rib, a condition known as costoclavicular syndrome arises. This disorder is thought to be one of the leading causes of TOS.
Provocation tests such as the Adson maneuver (scalenes), ‘Hands-up’ (pec minor), Allen (radial pulse) and the Elevation maneuver for costoclavicular canal impingement may be useful in identifying the pain producing site. These assessments may or may not reproduce symptoms, but are sometimes helpful in ruling out other causes, which may produce similar symptoms. Due to the overlapping of symptoms, it’s often difficult to make a definitive assessment using provocation tests. If in doubt, start treating proximally (neck & upper ribs) and release all possible impingement sites through the arms and hands.
Commonly seen muscle imbalance patterns such as Vladimir Janda’s upper crossed syndrome (Fig. 4) play a major role in the formation of entrapment neuropathies.
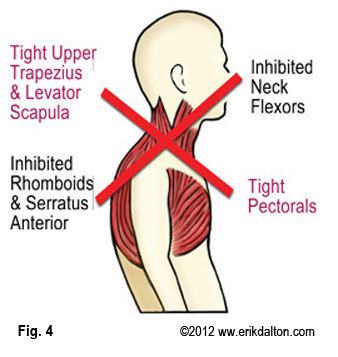 As tight pectoral muscles roll the shoulder girdle forward on the ribcage, the clavicles drop onto the first thoracic rib causing brachial plexus compression. Anterior displacement of the humeral head (tight pecs and lats) is also an area of impingement associated with upper crossed patterns. Fortunately, many illusive TOS cases are easily corrected using massage techniques such as those shown in the video below.
As tight pectoral muscles roll the shoulder girdle forward on the ribcage, the clavicles drop onto the first thoracic rib causing brachial plexus compression. Anterior displacement of the humeral head (tight pecs and lats) is also an area of impingement associated with upper crossed patterns. Fortunately, many illusive TOS cases are easily corrected using massage techniques such as those shown in the video below.
Successful long-term alleviation of pain, numbness, swelling, and paresthesias associated with this troublesome disorder requires that all upper quadrant postural asymmetries (slumped shoulders, forward heads, hyperkyphosis, etc.) be corrected prior to releasing smaller ‘impinging’ muscles such as intertransversarii, scalenes, and subclavius. Because the shoulder and neck area consist of very complex body parts with muscles and connective tissues going in all possible directions, therapists must focus intent on correcting postural strain patterns prior to chasing the pain. A thorough history, postural evaluations and appropriate corrections will help eliminate entrapment sites that irritate the brachial plexus and cause pain.
On sale this week only!
Save 25% off the Upper Body Course!

NEW! Enhanced video USB format!!!
Learn unique approaches to work with the shoulder girdle, arms, neck, and torso, this course will prepare you to relieve painful myoskeletal issues in the upper body. Through video demos and animation, you’ll learn to identify several compensatory movement patterns and their associated reflexogenic pain. With this understanding of where the true source of problems arise, you’ll be able to develop highly effective treatment protocols and deliver lasting results. This course provides you with the skills you need to confidently relieve pain issues in the upper body. (20 CE)
Bonus: When you order the Home Study version, get the eLearning course and and an additional 2CE Ethics eCourse for free!
Save 25% off the Upper Body Course this week only. Offer expires Sunday, March 1st. Click the button below for more information and to purchase the course for CE hours and a certificate of completion to display in your office.







